


A 56-year-old woman presented to our clinic with a 3-week history of atraumatic, progressive left shoulder pain with insidious onset. She had a medical history of hyperhomocysteinemia, heterozygous methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism discovered through genetic screening for cardiovascular risk, and hyperlipidemia. She reported no use of oral steroids, family history of osteonecrosis, alcohol abuse, or traumatic injury. She had a surgical history positive for a fracture of the left tibia and fibula treated with an intramedullary rod, a left bunionectomy, 2 cesarean sections, a hysterectomy, and an appendectomy. She had recently started taking methylated B2, fish oil, vitamin D, and a multivitamin, and she had allergies to Ceftin (cefuroxime axetil), codeine, and Dilaudid (hydromorphone). Before presentation, she had received acupuncture treatments to address the shoulder pain. She had a noncontributory family history and reported not having any relatives with Gaucher disease or sickle cell anemia. She worked as a transplant nurse and did not smoke or abuse alcohol.
On physical examination, the patient was found to have normal scapular posture and motion. She had a normal examination on the contralateral unaffected shoulder with intact forward elevation to 160°, abduction, external rotation, and internal rotation to the thoracolumbar junction. On the left side, she had forward elevation to 155°, intact abduction, external rotation, and internal rotation to the lumbosacral junction. Furthermore, she had difficulty with the abdominal compression test and also had a tight posterior capsule. On examination, she was motor sensory intact distally and did not have any focal motor sensory deficits. She reported mild discomfort with deep palpation of the long head of the biceps tendon in the bicipital groove and experienced no crepitus with range of motion of the shoulder.
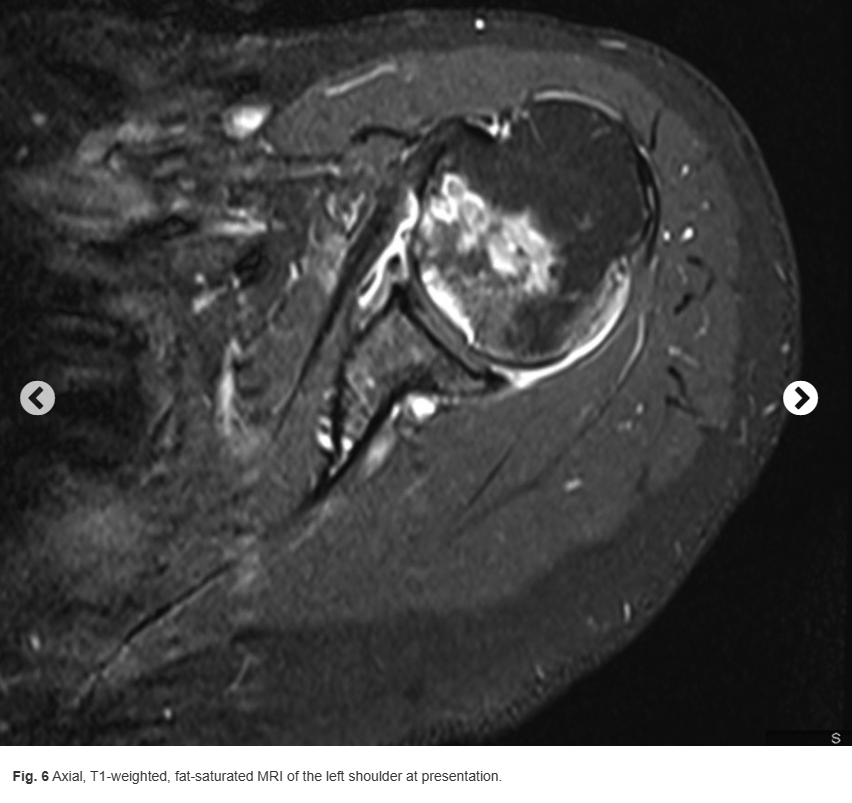
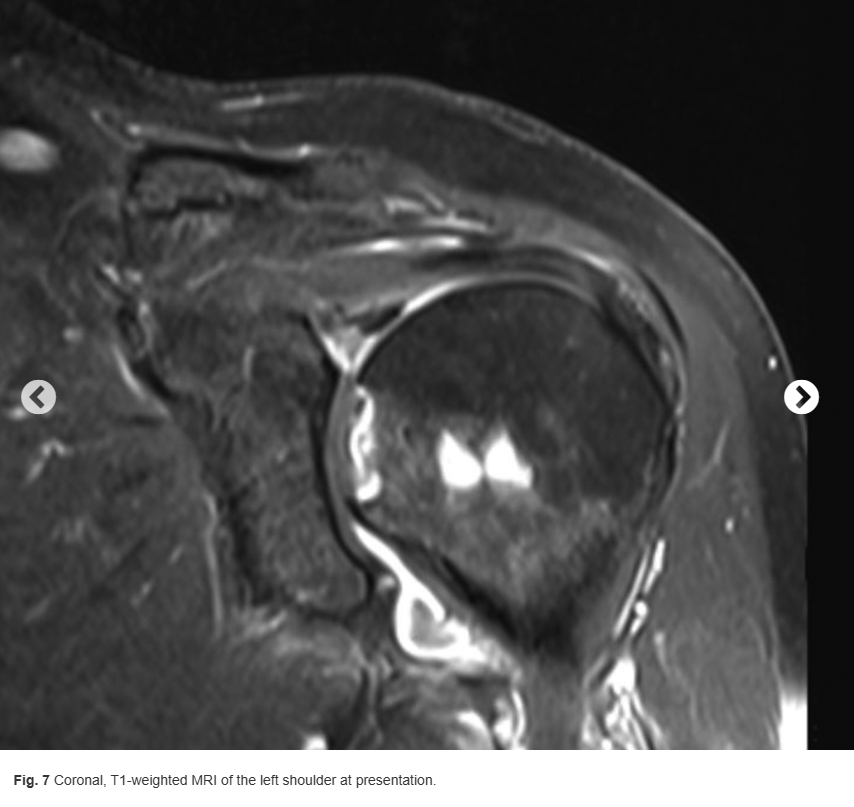
Her initial radiographs, taken at the initial clinic visit, demonstrated mild arthrosis of the acromioclavicular joint (Figs. 1 and 2). Her magnetic resonance imaging (MRI) scans, which were performed at another institution about 2 weeks before presentation at our institution, are shown in Figures 3 through 8.






What is the diagnosis?

