


A 9-week-old girl was brought to the emergency room by her grandmother, who stated that the child was not moving her right arm. There was no known history of trauma. The patient had been afebrile and feeding regularly and had regular wet diapers and stooling. She was born full term without complications, was up to date on vaccinations, and had no other notable medical history. On examination, her vital signs were normal and she was in no distress. She was normocephalic with normal respiratory effort. Her right wrist was swollen and elicited a pain response with palpation. There were no other deformities of her extremities and no skin lesions.
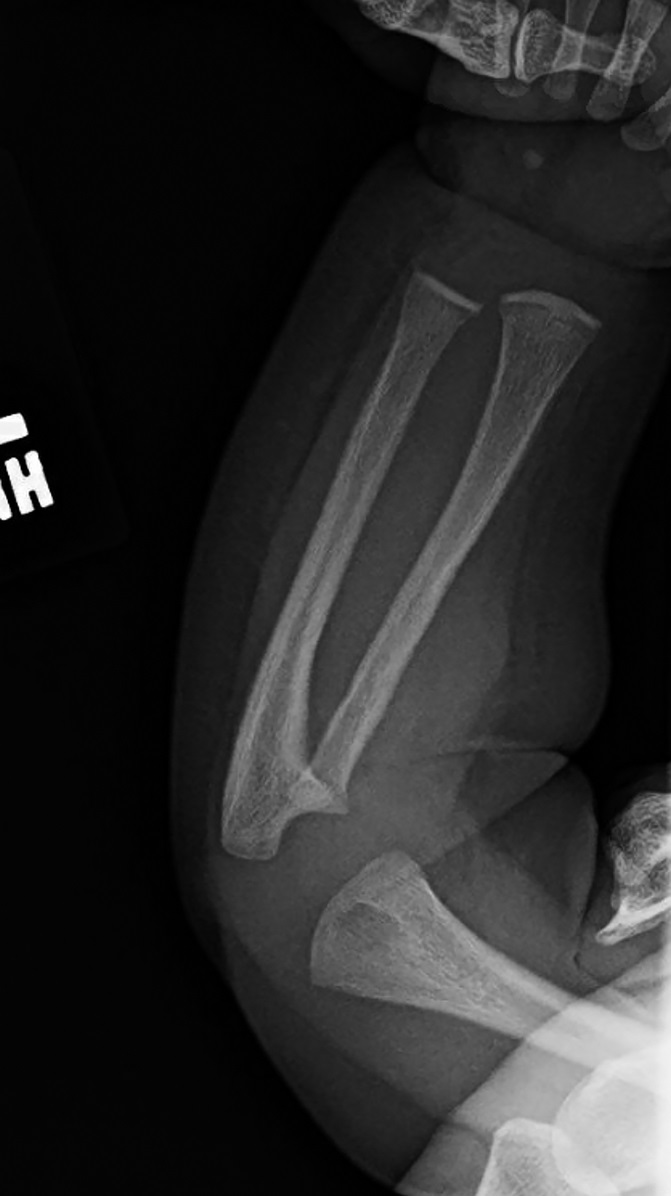
A radiograph of the right wrist was made and showed a subacute metaphyseal corner fracture of the distal part of the radius (Figs. 1-A and 1-B). Given the age and radiographic findings, a non-accidental trauma workup was initiated, per the institutional protocol. This included a computed tomographic (CT) scan of the head, abdomen, and pelvis, skeletal survey, blood work, and consultation to ophthalmology, general surgery, social work, Child Protective Services, and orthopaedics. The orthopaedic team evaluated the patient and placed the right arm in a soft immobilization, given the presumed subacute nature of the fracture. All other workup was negative, but, given the high suspicion for non-accidental trauma, the child was admitted and was subsequently discharged to foster care.




The patient was seen by a pediatrician 1 week later, and a repeat skeletal survey showed increased lucency of the right radius, interpreted as a “healing response to known fracture” (Figs. 2-A and 2-B). There was also a note of a “questionable periosteal reaction along the shaft of the right tibia” (Figs. 3-A and 3-B). Orthopaedics was not re-engaged after these findings, and the patient returned to the foster home.





Subsequently, the patient was tested and a rapid plasma reagin (RPR) screen was positive. The patient was brought to the Emergency Department, and a complete blood count (CBC), comprehensive metabolic panel, and cerebrospinal fluid (CSF) testing were obtained. The results were positive for transaminitis, hyperkalemia, and anemia. The CSF test was positive for venereal disease research laboratory (VDRL) testing. The patient was admitted to the Pediatrics Department, an infectious disease consultation was obtained, and the patient was administered intravenous benzathine penicillin G (BPG).
Repeat forearm radiographs were made 1 week later; these showed progressive lucency of the radius with osteolysis and cortical destruction (Figs. 4-A and 4-B). In addition, there were lesions noted in the left radius and ulna as well (Figs. 5-A and 5-B). The forearm was not further immobilized, and the patient was followed clinically by our orthopaedics team. The patient remained in the hospital to complete her course of antibiotics.









What is the diagnosis?


