


1. Introduction
The World Confederation of Physiotherapy (WCPT) [1] considers that physiotherapists are trained to meet the functional needs of people with disabilities. They also play a vital role in preventing and reducing health problems associated with disability. In and of itself, according to the American Physical Therapy Association (APTA), physiotherapy is a profession directed to the care of the individual, their family, and their community and focuses on the study and analysis of human body movement in order to improve the individual’s quality of life and contribute to their social development [2]. In this way, physiotherapists, in addition to their role in secondary and tertiary interventions, also participate in the identification of risks and behaviours that prevent or hinder the optimal development of human movement. In addition, they also take part in health promotion interventions, enabling people to have greater control over the determinants of health [3].
Regarding the functions of a physiotherapist, in Spain, the assistance function is the most important, with physiotherapists forming part of a multidisciplinary team. In general, the assistance function consists of the direct relationship that a physiotherapist maintains with a healthy/sick individual or society in order to prevent, cure, and recover injuries through professional actions, consisting of establishing, applying, and evaluating the methods, actions, and techniques of physiotherapy. A physiotherapist establishes a relationship with a healthy or sick individual in the psychological, communicative, and physical dimensions via physical means [4]. The Spanish public health system has just over 5000 physiotherapists, a ratio of 0.1 per 1000 inhabitants, far below the recommendations of the World Health Organization (WHO) of 1 physiotherapist per 1000 inhabitants [5]. Approximately 90% of Spanish physiotherapists work in the private sector, representing a ratio of 0.9/1000 inhabitants [6]. The Spanish public physiotherapy service has long waiting lists, and private sector interventions are not refunded by the public system. In terms of access to physiotherapy services through public health systems and the co-payment or lack thereof of said services, these vary widely in Europe [7].
According to a Global Burden of Disease Study in 2019 [8], musculoskeletal disorders ranked first in terms of years lived with disability. Physiotherapists have an important role in treating and preventing disability [1]. The prevalence of musculoskeletal disorders is very high in the elderly, being an important cause of pain, which can influence mood, physical functioning, physical inactivity, and social interaction and be a cause of a sedentary lifestyle [9]. Promotion of physical activity among the elderly plays a key role in healthy aging and may also have an impact beyond functionality, influencing mental health, quality of life, and well-being [10,11,12]. Previous evidence shows that subjective well-being is associated with reduced risk of all-cause mortality and incidence of specific conditions [13]. Physiotherapy can help society in the prevention and treatment of activity limitations and/or participation restrictions [12] in people at risk of movement disorders that, if not adequately prevented or treated, could lead to reduced physical activity, a lower quality of life, and a more sedentary lifestyle, which are associated with certain types of diseases and, consequently, an increased risk of mortality [9].
To the best of our knowledge, in Spain, no study has previously analysed the association between physiotherapy care and mortality in the general population. However, previous studies have associated certain physiotherapy interventions with a decrease in the risk factors associated with higher mortality [10,13,14,15]. The aim of this study was to analyse the association between attendance of physiotherapy and mortality in the general population from all causes after six years and describe the profile of patients who do not visit a physiotherapist in Spain, using the 2011/2012 National Health Survey.
2. Materials and Methods
2.1. Study Design
This was a population-based retrospective linkage cohort study. The baseline variables were collected from the Spanish National Health Survey 2011/2012 (ENSE11) [16] data source. The response variable was mortality from any cause (yes/no), obtained by crossing the ENSE11 database and the national database of deaths ordered by cause of death. This linkage was carried out by the National Institute of Statistics (INE) [17] through a probabilistic cross-link based on name, surname, date of birth, sex, personal identification number, and province of birth, using the Levenshtein distance metric, with a linkage quality higher than 97%. The linkage was carried out between the years 2011 and 2017, establishing the duration of follow-up to measure mortality between the 1 July 2011 and the 31 December 2017, for a total follow-up period of 6.4 years.
2.2. Participants
The period of inclusion for the ENSE11 respondents was between July 2011 and June 2012, covering a total of 21,007 adults (15 years and over). The ENSE11 has a national geographic scope and used a stratified three-stage sampling design. The units of the first stage were the census sections (population units of about 5000 inhabitants), the second-stage units were family dwellings, and, within each household, the third-stage units were adults aged 15 or over. A different sample was designed for each of the 17 regions of Spain, and was stratified by the size of the municipality. The survey represents all adults residing in Spain in 2011, about 39.7 million people. The present study included all ENSE11 adult participants and excluded those for whom information on the study variables was not available.
2.3. Variables/Outcomes Measures
The outcome variable was mortality from any cause (yes/no). The exposure variable was to answer question 52 of the ENSE11: “During the previous 12 months, have you visited a physiotherapist for yourself? (yes/no)”. The explanatory variables, which were considered potentially confounding, included five types:
- Socio-demographic variables: sex, age group, autonomous community of residence, size of municipality, social working class [18], body mass index, country of birth, marital status, educational level, and net monthly household income.
- Lifestyle habits: dental hygiene, tobacco use, exposure to tobacco smoke, risk of alcohol consumption, sleeping hours, main daily activity, and main leisure activity.
- Diet: breakfast, consumption of fruit, vegetables, legumes, dairy products, cakes and pastries, and fast food.
- Health and comorbidities: self-perceived health, presence of any chronic disease, high blood pressure (HBP), acute myocardial infarction (AMI), other heart disease, varicose veins in the legs, osteoarthritis, arthritis or rheumatism, chronic cervical pain, chronic low back pain, chronic allergy, asthma, chronic bronchitis, emphysema or chronic obstructive pulmonary disease (COPD); diabetes, stomach ulcer or duodenum, urinary incontinence, high cholesterol, cataracts, chronic skin problems, chronic constipation; cirrhosis or liver dysfunction; chronic depression; chronic anxiety; other mental problems; embolism, cerebral infarction or cerebral haemorrhage (stroke); migraine or frequent headache; haemorrhoids; malignant tumours; osteoporosis; thyroid problems; permanent injuries or defects caused by an accident or accidents in the previous year; mental health (GHQ12); use of glasses or contact lenses; use of hearing aids; flu vaccine in the last campaign; activity restriction (limitation of activity for health reasons in the previous two weeks); being bedridden for medical reasons in the previous two weeks; and limitation of daily activity in the previous six months.
- Use of health services: hospital admission in the previous year; visit to the primary care doctor in the previous month; visit to the specialist doctor in the previous month; visit to the day hospital in the previous year; visit to the psychologist in the previous year; and diagnostic tests performed in the previous year (X-ray; computed tomography scan (CT); ultrasound; nuclear magnetic resonance (MRN)).
of the additional materials details the code of the survey question that collects the information for each variable as well as the answer options. All information collected through the survey is self-reported by the responder at the time of the survey.
2.4. Statistical Analysis
A descriptive analysis of all the variables was carried out by calculating frequencies for the qualitative variables. The factors associated with the visit to the physiotherapist and the incidence of mortality were analysed using contingency tables, applying the chi-squared test. As crude measures of association, we calculated the cumulative incidence (CI) of mortality in the exposed group (Ie) and the incidence in the unexposed group (Iu), the unadjusted relative risk (RRc) value as the ratio of cumulative incidence (RRc = Ie/Iu), absolute risk reduction (ARR) as the difference in incidence (ARR = Iu − Ie), relative risk reduction (RRR) as complementary to RR (RRR = 1 − RR), and exposure impact number (EIN) as the inverse of ARR (EIN = 1/ARR), interpreted as the number of individuals with exposure among whom one excess case is due to the exposure [19].
To estimate the magnitudes of associations with incidence of mortality, adjusted relative risks (RRa) have been estimated together with their 95% confidence intervals, by adjusting multivariate Poisson models with robust variance [20]. A stepwise variable selection procedure was carried out based on the Akaike information criterion (AIC), and the possible confusion of the explanatory variables by the effect of visiting the physiotherapist on the incidence of mortality was evaluated. The possible multicollinearity of the variables was also taken into account. A model validation process was carried out, dividing the sample randomly into two subsamples: training to adjust the model (70% of the total) and testing to validate it (30% of the total), obtaining an honest estimate of the predictive capacity of the model using the area under the ROC curve and its 95% confidence interval in the testing sample. To obtain representative estimates of the Spanish population, complex sampling was taken into account, using the survey elevation factor divided by its mean as a weighting factor, obtaining weights centred on its mean [21]. The analyses were performed using SPSS v.28 [22] and R v.4.0.2 software [23].
3. Results
Of the total of 21,007 adults (15 years or older) surveyed, 18 (0.08%) participants were excluded for not presenting values in the exposure variable (visit to the physiotherapist) and 592 (2.8%) subjects for not presenting valid values in the rest of the explanatory variables, obtaining a total of 20,397 participants for analysis. Figure 1 shows the study flow chart.
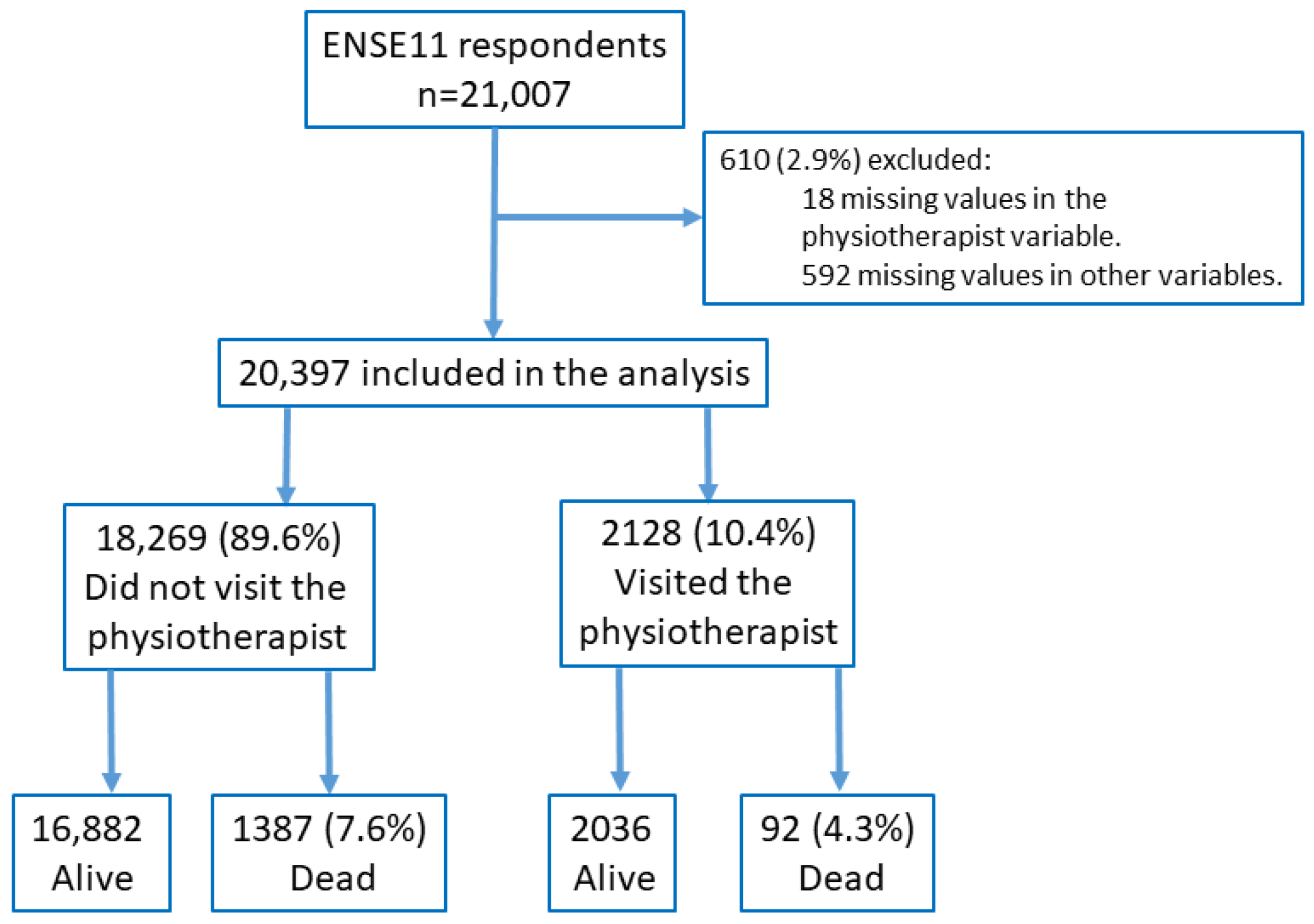
Figure 1. Flow chart of the study.
Of the 20,397 participants included in this study, 5.4% (n = 1101) visited the physiotherapist the previous year, 51.3% (n = 10,455) were women, 85.7% (n = 17,470) were born in Spain, 15.4% (n = 3144) had obesity, 33.6% (n = 6848) had secondary education, 45.1% (n = 9199) reported standing most of the day, 44.4% (n = 9051) did not perform any physical leisure activity, 51.0% (n = 10,413) rated their self-perceived health as good, 18.3% (n = 3734) had osteoarthritis, 27.3% (n = 5566) had an X-ray in the previous year, and 7.4% (n = 1513) had an MRI during the previous year. The description of the study sample according to the study variables is presented in in summary form ( in extended form).
The CI of total mortality was 5.4% (n = 1107) with a maximum follow-up of 6.4 years (mean follow-up of 6.2 years, with a total of 127,711 subject-years of follow-up). The incidence of total mortality in the group that visited the physiotherapist the previous year was 3.5% (n = 74) compared with 5.6% (n = 1033) of those who did not visit the physiotherapist (p < 0.001). The RRc was 0.62 (95% CI: 0.50–0.79), the RRR was 0.38 (95% CI: 0.21–0.50), and the EIN was 47.1 (95% CI: 33.5–79.0). shows other factors that were associated with all-cause mortality. Figure 2 shows the distribution of mortality by year.
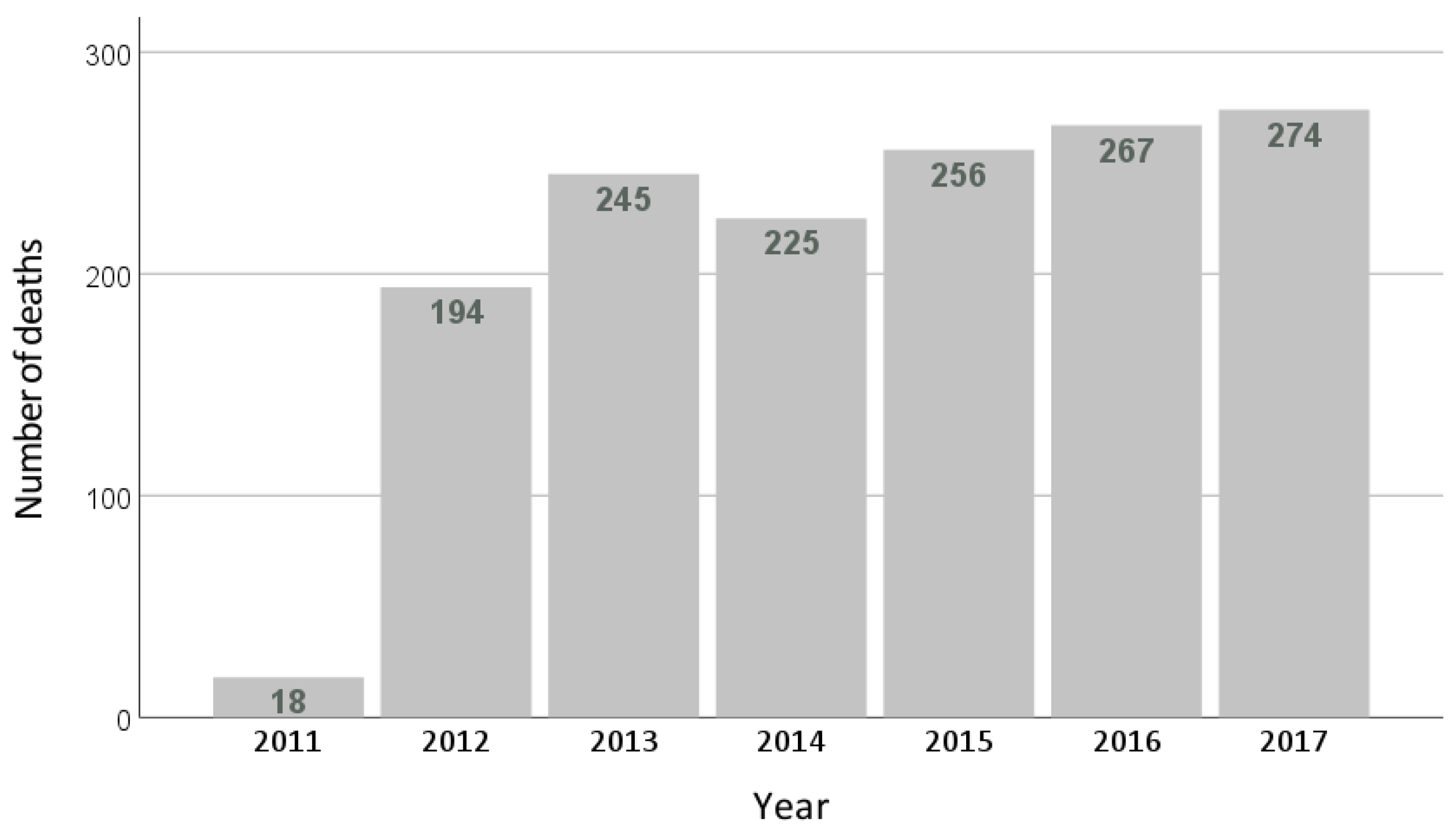
Figure 2. Distribution of mortality by year.
In the multivariate analysis, the RRa of total mortality in the group that visited the physiotherapist was 0.699 (95% CI: 0.528–0.927; p = 0.013), which means that visiting the physiotherapist was associated with lower all-cause mortality (quantified at 30.1%) compared with not visiting the physiotherapist. This estimation was adjusted for 28 variables . shows the estimation of the relative risk of death of the complete multivariate model.
and show the profile of study participants according to whether they visited the physiotherapist in the previous year. People belonging to the age group between 55–64 years went to the physiotherapist the most (11.9%; n = 318; p < 0.001), while those that went to the physiotherapist the least were 85 years or older (4.4%; n = 21; p < 0.001). People with obesity went to the physiotherapist less than people with normal weight (8.7%; n = 272; p < 0.001 vs. 11.4%; n = 1027; p < 0.001). Level of income was directly proportional to attendance at the physiotherapist, with higher attendance in the group with incomes over EUR 2251 and lower attendance in the group with incomes under EUR 800 (15.4% n = 491; p < 0.001 vs. 6.3% n = 172; p < 0.001). People who slept less than 7 hours a day went to the physiotherapist more than those who slept more than 9 hours a day (13.0%; n = 589; p < 0.001 vs. 7.2%; n = 88; p < 0.001). Regarding leisure physical activity, sedentary people went to the physiotherapist less (8.5%; n = 770; p < 0.001) than those who performed physical activity frequently (13.8%; n = 368; p < 0.001) and those who performed sports training (17.4%; n = 337; p < 0.001). People who rated their health as poor (17.0%; n = 209; p < 0.001) or very poor (15.8%; n = 47; p < 0.001) went to the physiotherapist more than those who rated it as good (9.8%; n = 1017; p < 0.001) or very good (6.1%; n = 270; p < 0.001). Not having a chronic disease was associated with not having visited a physical therapist (8.5%; n = 1005; p < 0.001). Likewise, not having presented any physical limitation during the previous two weeks was also associated with not having visited the physiotherapist (9.2%; n = 1658; p < 0.001). Regarding the use of health services, people without hospital admission in the previous year (9.6%; n = 1788; p < 0.001), those who did not visit the general practitioner in the previous month (9.6%; n = 1408; p < 0.001) or the specialist physician (8.7%; n = 1513; p < 0.001), and those who did not attend a day hospital in the previous year (9.7%; n = 1836; p < 0.001) visited the physical therapist less than those who used these health services.
4. Discussion
The present study shows an association between visiting the physiotherapist and all-cause mortality at six years (quantified at 30% and adjusted for 28 variables from all the blocks of the survey: sociodemographic, lifestyle, health and comorbidities, and use of health services). In addition, this study shows that the factors associated with not visiting the physiotherapist were being aged 75 years or older, having obesity, having a low income (less than EUR 800), sleeping more than 9 hours, being sedentary, having a very good self-perceived health state, not suffering from a chronic illness or not having presented any physical limitation in the two weeks before being surveyed, and not having been admitted to hospital or visited a day hospital during the previous year or having visited the general practitioner or a specialist during the previous month.
Consistent with other previous works, this study identified differences regarding the profile of the physiotherapy patients, such as certain comorbidities, the operation of the health system making the physiotherapy service available, educational level, and the presence of serious conditions [24,25]. According to Anderson [26], variability in terms of healthcare would be appropriate when it is due to the patient’s clinical health condition, but it is questionable to consider whether variation is appropriate when it is due to factors such as social structure, beliefs about health, or accessibility. For example, our study found that people with low incomes visited the physiotherapist less than people with high incomes. This might be due to the saturation of the public health system and the limitation of paying for a private service [6]. Removing any inappropriate variation is necessary to improve the quality of physiotherapy care [27], and, for this, factors associated with not receiving physiotherapeutic care first need to be identified, as we have explored in the present study, in order to take steps in this regard and develop new strategies to improve access to this service.
Currently, increased participation in sports and physical exercise is widely promoted as an approach to a physically active lifestyle that has a positive effect on healthy aging. This has caused a higher incidence of sports-related injuries [28] and a greater presence of these patients at the physiotherapist’s consulting room as reflected in the results of this study. However, according to our results, sedentary and obese people visited the physiotherapist less than people with a normal weight.
In our study, working-age individuals went to the physiotherapist more often than the non-working-age population. According to other research, the working-age population exhibits a high incidence of musculoskeletal injuries, being the main reason for them to receive medical attention, hospitalisations, emergency visits, physical rehabilitation, and physiotherapy [29].
Some of the main physiotherapy interventions developed in the prevention and promotion of health and that may be related to improvement in certain health states that are indirectly associated with a reduction in all-cause mortality include:
- (A)
- Improvement in self-perceived health and quality of life:
In a systematic review conducted in 2008, greater well-being was associated with lower all-cause mortality in initially healthy population cohorts (adjusted hazard ratio 0.82, 95% confidence interval 0.76 to 0.89) [30]. Subsequently, several studies documented protective associations between various measures of subjective well-being and mortality [31,32]. In the elderly with good mobility, this association may be irrespective of age, sex, educational level, marital status, and drug use [33].
Quality of life among the elderly becomes poorer as they get older, and, consequently, so does their subjective well-being, partly due to health deterioration with the appearance of chronic diseases and, especially, the progressive loss of functionality [34]. In this regard, the promotion of physical activity among the elderly plays a key role in healthy aging, possibly representing an impact beyond functionality, affecting mental health and quality of life. The WHO warns that physical inactivity is a major risk factor that causes the most deaths, ranking fourth behind HBP, tobacco, and hyperglycaemia [35]. This means that physical inactivity is the cause of 6% of deaths recorded worldwide. According to Blair [36], physical inactivity is one of the most important public health problems in the twentieth century. Physiotherapy might have a differential impact on the maintenance and improvement of self-perceived health through the promotion of health and well-being, prevention of limitations and restrictions on activity, and social participation in people with movement disorders [36]. According to this study, people who rated their health as poor or very poor visited the physiotherapist more often; this fact could be a turning point.
Chronic degenerative musculoskeletal pathologies inherent in age constitute one of the fundamental causes of loss of functional independence. Being able to re-establish an adequate condition to maintain optimal and adapted functionality has proven to be essential in the maintenance of functional capacity and is closely related to life expectancy and mortality [37]. In this regard, physiotherapists are healthcare professionals, often the first choice and easily accessible in the private sector, trained for the management and proper treatment of musculoskeletal injuries [38]. This study reported that those patients who suffered from a chronic degenerative disease such as osteoarthritis, chronic cervical pain, chronic low back pain, or osteoporosis resorted to physiotherapy more regularly.
In many cases, physiotherapists will be in charge of the treatment of musculoskeletal disorders or other types of injuries, prescribing adapted therapeutic exercises minimising or reducing the sedentary lifestyle caused by such disorders. Sometimes they will ensure quick referral to other healthcare professionals and detect red flags that require urgent attention [38]. A physiotherapist’s ability to identify clinical signs of danger (i.e., detection of red flags) and understand when patients should be referred to a physician is vital to patient safety [39]. It has been reported that physiotherapists diagnose with the same accuracy as orthopaedic surgeons, as sports medicine doctors [40], in patients with musculoskeletal disorders [41], and as general practitioners in the UK [42]. In some situations, physiotherapists can contribute to patient safety by identifying the presence of a wide range of systemic diseases and various pathologies requiring medical management.
Falls represent one of the main causes of injury, functional impairment, repeated visits to the physician, readmission to hospital, and mortality in people aged 65 and over [43,44]. In addition, decreased mobility during hospitalisation is associated with loss of muscle mass, increased potential risk of falls, functional decline, and increased mortality, especially in the elderly [45,46]. Promoting mobility soon after an intervention potentially decreases the risk of falls [47]. Falls that do not result in physical injury can also have serious implications [48]. Exercise and physiotherapy interventions are shown to be very effective in preventing falls [44,49,50]. Despite this, people over 65 years visited the physiotherapist less than other age groups in this study. Thus, it is important to facilitate access to the physiotherapist for this age group.
Visiting the physiotherapist does not directly reduce mortality, but, in certain situations, it may modify intermediate health states that indirectly reduce total mortality, acting as a positive mediator between certain health/disease states and total mortality. Knowing the determinant factors related to physiotherapist access could help to develop intervention strategies to improve access to this type of health care and analyse whether these strategies are effective and can represent greater protection against mortality in physiotherapy patients through properly designed prospective studies.
Limitations
The present study has some limitations that should be considered. The data on the exposure and explanatory study variables are from the respondents’ self-reported information, a fact that could generate a recall bias. However, previous studies that compared patients’ answers in questionnaires against the data from medical records showed a high degree of sensitivity and agreement [51]. Similarly, self-reported chronic diseases have been considered a source of useful information for prevalence studies and have been validated [52]. Likewise, the data were obtained from information collected in the ENSE16, which has national and regional representation and constitutes one of the largest data collection programs of the Spanish Ministry of Health, whose results have been validated and are considered an essential element of territorial cohesion for population monitoring. The official data from the INE have been analysed, being a comprehensive population sample for all the years under study [17]. However, the ENSE11 only provides information on attendance at physiotherapy treatment, but not on frequency, subsequent visits, or reasons for visiting the physiotherapist. Information about external factors, such as government education campaigns or changes in health spending, that might potentially have had an impact on mortality, were not included either in the study analysis.
5. Conclusions
Visiting the physiotherapist was associated with lower mortality from all causes in the population living in Spain. Factors associated with not visiting the physiotherapist were being 75 years of age or older; being obese; having a low income (less more than EUR 800); sleeping more than 9 h; being sedentary; having a very good self-perceived health state; not suffering from a chronic illness or not having presented any physical limitation in the two weeks prior to being surveyed; not having been admitted to hospital or visited a day hospital during the previous year; and not having visited the general practitioner or a specialist during the previous month.
References
- World.physio. Available online: https://world.physio/sites/default/files/2021-05/PS-2019-Disability-Spanish.pdf (accessed on 24 October 2022).
- American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. American Physical Therapy Association. Phys. Ther. 2001, 81, 9–746. [Google Scholar]
- Pan American Health Association. Carta de Ottawa para la Promoción de la Salud. Available online: https://www.paho.org/hq/dmdocuments/2013/Carta-de-ottawa-para-la-apromocion-de-la-salud-1986-SP.pdf (accessed on 10 July 2022).
- Gallego Izquierdo, T. Bases Teóricas y Fundamentos de la Fisioterapia; Médica Panamericana: Buenos Aires, Argentina; Madrid, Spain, 2007. [Google Scholar]
- Practising Physiotherapists, per 100,000—Eurostat Statistics Explaned. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Practising_physiotherapists,_2020_(per_100_0000_inhabitants)_Health2022.png (accessed on 10 July 2022).
- Fernández-Lago, H.; Climent-Sanz, C.; Bravo, C.; Bosch-Barceló, P.; Masbernat-Almenara, M.; Sanjuan-Sánchez, D.; Briones-Vozmediano, E. Physiotherapists’ experiences on assisting physiotherapy users during the COVID-19 pandemic with lockdown measures in Spain. Physiother. Res. Int. 2023, 28, e2015. [Google Scholar] [CrossRef] [PubMed]
- Martínez-López, J.Á.; Martínez-Gayo, G. Consequences of the Increase of the Pharmaceutical Copayment in Spain: A New Material Deprivation. Convergencia 2019, 26, 1–21. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Hadjistavropoulos, T.; Herr, K.; Turk, D.C.; Fine, P.G.; Dworkin, R.H.; Helme, R.; Jackson, K.; Parmelee, P.A.; Rudy, T.E.; Beattie, B.L.; et al. An interdisciplinary expert consensus statement on assessment of pain in older persons. Clin. J. Pain. 2007, 23 (Suppl. S1), S1–S43. [Google Scholar] [CrossRef] [PubMed]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef]
- Fundadeps.org. Available online: https://fundadeps.org/wp-content/uploads/eps_media/recursos/documentos/267/libro_ejercicio_cardiosaludable_CSD.pdf (accessed on 24 October 2022).
- World Health Organization. Musculoskeletal Health. Available online: https://www.who.int/es/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 15 July 2022).
- Barger, S.D.; Broom, T.W.; Esposito, M.V.; Lane, T.S. Is subjective well-being independently associated with mortality? A 14-year prospective cohort study in a representative sample of 25 139 US men and women. BMJ Open 2020, 10, e031776. [Google Scholar] [CrossRef]
- Gentil, P.; de Lira, C.A.B.; Vieira, C.A.; Ramirez-Campillo, R.; Haghighi, A.H.; Clemente, F.M.; Souza, D. Resistance Training before, during, and after COVID-19 Infection: What Have We Learned So Far? Int. J. Environ. Res. Public Health 2022, 19, 6323. [Google Scholar] [CrossRef]
- Momma, H.; Kawakami, R.; Honda, T.; Sawada, S.S. Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: A systematic review and meta-analysis of cohort studies. Br. J. Sports Med. 2022, 56, 755–763. [Google Scholar] [CrossRef]
- National Institute of Statistics. National Health Survey. 2011. Available online: https://www.ine.es/metodologia/t15/t153041912.pdf (accessed on 22 October 2022).
- National Institute of Statistics. Deaths by Death Cause. 2022. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176780&menu=ultiDatos&idp=1254735573175 (accessed on 22 October 2022).
- Álvarez-Dardet, C.; Alonso, J.; Domingo, A.; Regidor. La Medición de la Clase Social en Ciencias de la Salud; Sociedad Española de Epidemiología: Barcelona, Spain, 1995. [Google Scholar]
- Heller, R.F.; Dobson, A.J.; Attia, J.; Page, J. Impact numbers: Measures of risk factor impact on the whole population from case-control and cohort studies. J. Epidemiol. Community Health 2002, 56, 606–610. [Google Scholar] [CrossRef]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Beneyto, M.; Nolasco, A.; Moncho, J.; Pereyra-Zamora, P.; Tamayo-Fonseca, N.; Munarriz, M.; Salazar, J.; Tabarés-Seisdedos, R.; Girón, M. Psychometric behaviour of the strengths and difficulties questionnaire (SDQ) in the Spanish national health survey 2006. BMC Psychiatry 2013, 13, 95. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 28.0, Released 2021; IBM Corp Computing: Armonk, NY, USA; Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 22 October 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 22 October 2022).
- Rabah, N.M.; Knusel, K.D.; Khan, H.A.; Marcus, R.E. Are There Nationwide Socioeconomic and Demographic Disparities in the Use of Outpatient Orthopaedic Services? Clin. Orthop. Relat. Res. 2020, 478, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.A.; Onega, T.; Weeks, W.B.; Lurie, J.D. Where the United States spends its spine dollars: Expenditures on different ambulatory services for the management of back and neck conditions. Spine 2012, 37, 1693–1701. [Google Scholar] [CrossRef]
- Anderson, J.G. Health services utilization: Framework and review. Health Serv. Res. 1973, 8, 184–199. [Google Scholar]
- Hannan, T.J. Variation in health care--the roles of the electronic medical record. Int. J. Med. Inf. 1999, 54, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Minoves Font, M. Clinical applications of nuclear medicine in the diagnosis and assessment of musculoskeletal sports injuries. Rev. Esp. Med. Nucl. Imagen Mol. (Engl. Ed.) 2020, 39, 112–134, (In English, Spanish). [Google Scholar] [CrossRef]
- Ruesga, S.M.; Vasco, D.C.; Gómez, V.; Monsueto, S.E.; Nestares, C.R.; Bichara, J.S. Work accident mutuals and the management of temporary disability [Internet]. Seg-social.es. Available online: https://www.seg-social.es/wps/wcm/connect/wss/1e437183-27ec-439b-afa1-4faa23c90f7c/F45_1_07.pdf?MOD=AJPERES (accessed on 24 October 2022).
- Chida, Y.; Steptoe, A. Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosom. Med. 2008, 70, 741–756. [Google Scholar] [CrossRef]
- Gana, K.; Broc, G.; Saada, Y.; Amieva, H.; Quintard, B. Subjective wellbeing and longevity: Findings from a 22-year cohort study. J. Psychosom. Res. 2016, 85, 28–34. [Google Scholar] [CrossRef]
- Lawrence, E.M.; Rogers, R.G.; Wadsworth, T. Happiness and longevity in the United States. Soc. Sci. Med. 2015, 145, 115–119. [Google Scholar] [CrossRef]
- Trudel-Fitzgerald, C.; Kubzansky, L.D.; VanderWeele, T.J. A Review of Psychological Well-Being and Mortality Risk: Are All Dimensions of Psychological Well-Being Equal? In Interdisciplinary Perspectives from the Social Sciences and the Humanities; Oxford Academic: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between frailty and quality of life among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland; Available online: https://www.who.int/publications/i/item/9789241563871 (accessed on 24 October 2022).
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- World Physiotherapy. Policy Statement: Patient/Client Direct Access and Self-Referral to Physical Therapy [Internet]. Available online: http://www.wcpt.org/policy/ps-direct-access (accessed on 24 October 2022).
- Downie, F.; McRitchie, C.; Monteith, W.; Turner, H. Physiotherapist as an alternative to a GP for musculoskeletal conditions: A 2-year service evaluation of UK primary care data. Br. J. Gen. Pr. 2019, 69, e314–e320. [Google Scholar] [CrossRef] [PubMed]
- Welch, E. Red flags in medical practice. Clin. Med. 2011, 11, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Décary, S.; Fallaha, M.; Pelletier, B.; Frémont, P.; Martel-Pelletier, J.; Pelletier, J.P.; Feldman, D.E.; Sylvestre, M.P.; Vendittoli, P.A.; Desmeules, F. Diagnostic validity and triage concordance of a physiotherapist compared to physicians’ diagnoses for common knee disorders. BMC Musculoskelet. Disord. 2017, 18, 445. [Google Scholar] [CrossRef] [PubMed]
- Matifat, E.; Perreault, K.; Roy, J.S.; Aiken, A.; Gagnon, E.; Mequignon, M.; Lowry, V.; Décary, S.; Hamelin, B.; Ambrosio, M.; et al. Concordance between physiotherapists and physicians for care of patients with musculoskeletal disorders presenting to the emergency department. BMC Emerg. Med. 2019, 19, 67. [Google Scholar] [CrossRef]
- Vedanayagam, M.; Buzak, M.; Reid, D.; Saywell, N. Advanced practice physiotherapists are effective in the management of musculoskeletal disorders: A systematic review of systematic reviews. Physiotherapy 2021, 113, 116–130. [Google Scholar] [CrossRef]
- Miró, Ò.; Nayla Brizzi, B.; Aguiló, S.; Alemany, X.; Jacob, J.; Llorens, P.; Herrero Puente, P.; González Ramón, B.; Castro Jiménez, V.; Torres Machado, V.; et al. Profile of elderly patients seen in the emergency room due to falls (FALL-ER Registry): Magnitude of the problem and possibilities for improvement in hospital emergency services. Emergencies 2018, 30, 231–240. [Google Scholar]
- Cáceres Santana, E.; Bermúdez Moreno, C.; Ramírez Suarez, J.; Bahamonde Román, C.; Murie-Fernández, M. Incidence of falls in long-stay hospitals: Risk factors and strategies for prevention. Neurologia 2022, 37, 165–170. [Google Scholar] [CrossRef]
- Kanejima, Y.; Shimogai, T.; Kitamura, M.; Ishihara, K.; Izawa, K.P. Effect of Early Mobilization on Physical Function in Patients after Cardiac Surgery: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7091. [Google Scholar] [CrossRef]
- Coker, R.H.; Hays, N.P.; Williams, R.H.; Wolfe, R.R.; Evans, W.J. Bed rest promotes reductions in walking speed, functional parameters, and aerobic fitness in older, healthy adults. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Growdon, M.E.; Shorr, R.I.; Inouye, S.K. The Tension Between Promoting Mobility and Preventing Falls in the Hospital. JAMA Intern. Med. 2017, 177, 759–760. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Williams, C.S. The effect of falls and fall injuries on functioning in community-dwelling older persons. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, M112–M119. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.M.; Kamkar, N.; Pieruccini-Faria, F.; Osman, A.; Sarquis-Adamson, Y.; Close, J.; Hogan, D.B.; Hunter, S.W.; Kenny, R.A.; Lipsitz, L.A.; et al. Evaluation of Clinical Practice Guidelines on Fall Prevention and Management for Older Adults: A Systematic Review. JAMA Netw. Open 2021, 4, e2138911. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.; Doe, K.; Gerry, M.; Moore, B.; Wingood, M.; Renfro, M.; Gell, N. Outcomes of a Physical Therapist-Led, Statewide, Community-Based Fall Risk Screening. J. Geriatr. Phys. Ther. 2020, 43, 185–193. [Google Scholar] [CrossRef]
- Mac Donald, R.; Baken, L.; Nelson, A.; Nichol, K.L. Validation of self-report of influenza and pneumococcal vaccination status in elderly outpatients. Am. J. Prev. Med. 1999, 16, 173–177. [Google Scholar] [CrossRef]
- Martin, L.M.; Leff, M.; Calonge, N.; Garrett, C.; Nelson, D.E. Validation of self-reported chronic conditions and health services in a managed care population. Am. J. Prev. Med. 2000, 18, 215–218. [Google Scholar] [CrossRef]