


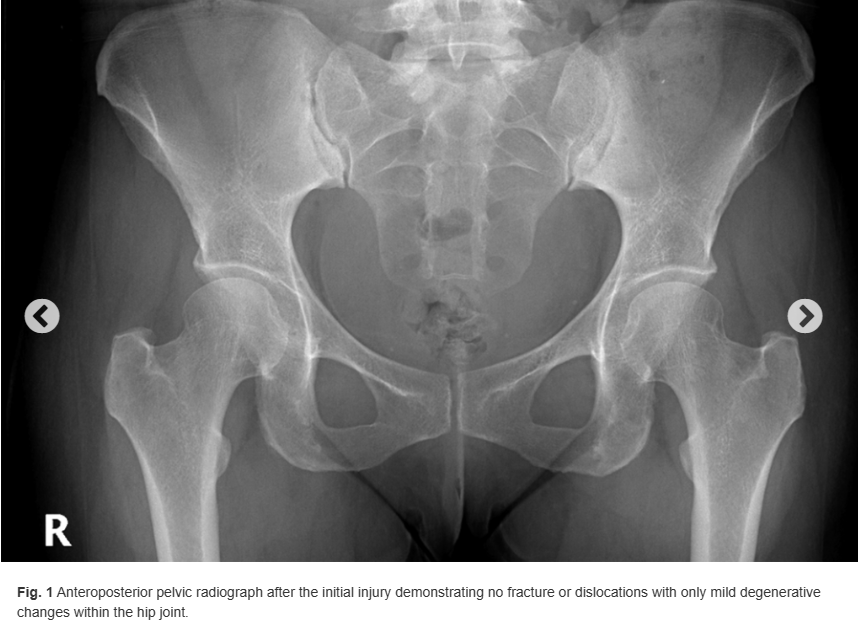
A 45-year-old woman initially presented to our orthopaedic clinic 5 weeks after an injury to the right hamstring. She was managed conservatively by a provider at an outside institution without satisfactory progress. Further workup at our institution included a pelvic radiograph, which showed no fracture or dislocations and only mild degenerative changes within the hip joint (Fig. 1). Her magnetic resonance imaging (MRI) scan revealed a 3-tendon tear of the right proximal hamstring with 3 cm of retraction. Given that she was an active individual and underwent failed conservative measures such as physical therapy and activity modification, the patient was deemed appropriate for surgical intervention.
One week later, the patient underwent open right proximal hamstring 3-anchor repair and sciatic nerve neurolysis. The procedure was uncomplicated. She reported good progress at her 3-week, 6-week, and 3-month postoperative appointments. The incision healed nicely without signs of infection. The patient was compliant with physical therapy, and, by 3 months, she had regained 4/5 hamstring strength and was able to actively flex the knee to 110°.
Six months after the operation, the patient returned to our clinic reporting worsening pain over the surgical site after slipping 5 days earlier. She described bruising and swelling in the region of the previous injury, and she was concerned that she had reinjured the hamstring. She reported that, before this episode, she had been doing extremely well and was back to nearly all activities. On examination, the incisions were well-healed and no ecchymosis was observed. There was no palpable defect along the proximal hamstring tendon or at the right ischial tuberosity, and the patient maintained her baseline 4+/5 hamstring strength on the injured side. No masses or other abnormalities were observed on examination. The patient also first mentioned at this visit that the contralateral hip had been bothering her for approximately 2 years. History and physical examination were consistent with external snapping hip.
Anteroposterior pelvic radiograph revealed symmetric densities within the soft tissue around the bilateral hips. This was initially suspected to be a radiographic artifact. Repeat radiographs were made, which showed the same symmetric opacities in the abductor region of both hips (Fig. 2). Additional history gathered from the patient revealed no plausible explanation for the radiographic findings, and examination of the area was unremarkable. The patient and provider’s concern and curiosity with regard to the unique appearance on imaging prompted further investigation, and, thus, colleagues in orthopaedic oncology and radiology were consulted. Unfortunately, no definitive explanation for the radiographic findings could be provided. Extensive laboratory work was ordered to investigate possible systemic causes of calcium deposition within the soft tissues including complete blood count with differential, comprehensive metabolic panel, serum protein electrophoresis, thyroid stimulating hormone, uric acid, 25-hydroxy vitamin D, calcium, erythrocyte sedimentation rate, C-reactive protein, and rheumatoid factor. With regard to the hamstring injury, examination suggested no evidence of a retear, so the patient was given a prescription for physical therapy to help to improve her flexibility and strength. Follow-up appointments for both the radiological findings and the hamstring injury were scheduled.

What is the diagnosis?